
Key points of extended radical resection for locally advanced lung cancer
Extended lung cancer resection involves vascular surgery, cardiac surgery, tracheal surgery and highly difficult thoracic surgery techniques. Only senior thoracic surgeons who have received training in general hospitals can fully master the above professional techniques. Therefore, whether the operation can be completed depends not only on the degree of tumor invasion, but also on the surgical skills of the surgeon. The following introduces some necessary surgical techniques for reference.
1. Treatment of the pulmonary artery trunk. If the tumor invades the root of the left pulmonary artery and the pulmonary artery trunk, the pericardium is cut longitudinally between the front of the hilum and the phrenic nerve. The incision is opened upwards first, and the fold of the pulmonary artery and pericardium is separated. The left pulmonary artery and part of the pulmonary artery trunk are freed. The free range should be more than 1.5 cm away from the edge of the tumor. Use a non-damaging vascular clamp to clamp the pulmonary artery trunk to no more than 1/2 of the diameter, and observe the changes in blood oxygen saturation, blood pressure, and heart rate (rhythm). Cut off the left pulmonary artery and part of the pulmonary artery trunk 5 mm away from the edge of the tumor, and use a non-damaging thread to suture and repair the broken ends continuously. For safety reasons, the method of cutting and suturing can be used.
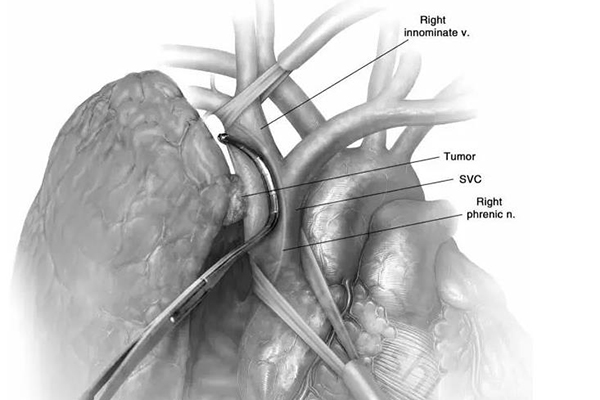
2. Treatment of the superior vena cava. If the vena cava is invaded, artificial blood vessels need to be replaced. Take a posterolateral incision to perform right upper lung resection. Fully dissect the left and right innominate veins and superior vena cava. Use a "Y"-shaped artificial blood vessel, anastomose the proximal end with the superior vena cava near the right atrium (or right auricle), and anastomose the distal end with the left and right innominate veins respectively. When the superior vena cava is removed, make preparations as much as possible in advance to reduce the time of vascular occlusion, which should generally be controlled within 30 minutes (blood pressure can be appropriately controlled during the occlusion period, and low-dose hormones can be used to reduce cerebral edema).
3. Invasion of the left atrium is divided into two situations: when the heart is not stopping beating and after the establishment of extracorporeal circulation: when the heart is not stopping beating, it is suitable for the lesion to invade the atrial wall to a small extent, and no patch is needed to restore the size of the atrium after removal. The method of suturing and cutting is adopted. The pericardial incision is extended to the trunk of the inferior pulmonary vein, the pericardium before and after the hilum is completely opened, and the superior and inferior pulmonary veins are dissected and freed. Use a non-invasive vascular clamp to clamp the left atrial wall 1 cm away from the tumor, observe that there is no change in blood pressure and heart rate, suture and knot the proximal side of the pre-cut line of the left atrial wall outside the clamp with a 4-0 prolene line, and partially cut off the atrial wall 5 mm away from the edge of the tumor (cut and sew), and use a non-damaging line to suture and repair the broken ends continuously. Pay attention to ensure that the two ends of the cut left atrial opening will not slip off and the vascular clamp buckle will not jump out. Then, gradually cut and suture the remaining part. For those with a larger area of invasion of the atrial wall or with cancer thrombus inside, extracorporeal circulation can be established, the tumor can be removed, and the left atrial wall can be repaired with a patch.

A case of locally advanced lung cancer (T4) invading the heart and large blood vessels was successfully treated with thoracoscopically assisted small incision surgery
Recently, a patient with locally advanced (T4) lung cancer invading the pericardium and large blood vessels underwent "VATS-assisted small incision left lung cancer radical resection". During the operation, the pulmonary artery trunk shaping + left atrium shaping were completed using a endoscopic linear cutter stapler device, and the operation went very smoothly. The use of such instruments makes this complex operation simple, safe and reliable. The patient's operation went smoothly, and he was able to get out of bed 16 hours after the operation and was discharged from the hospital 10 days after the operation.